A. Direct Acting:
Pilocarpine (natural alkaloid and a tertiary amine)
Bethanechol and Carbachol (synthetic drugs and quaternary amines)
Note: The tertiary amine are more lipid soluble and easily cross the blood brain barrier (BBB), while the quaternary amines are less lipid soluble and poor to cross BBB.
Mechanism of action: These drugs are direct agonists of muscarinic or nicotinic receptors or both at the target sites and produce their particular effects like contraction of smooth muscle, e.g in GI, respiratory tract and urinary bladder; and an increase of exocrine gland secretions, e.g. salivation and sweating.
B. Indirect Acting:
These are of two types: reversible or irreversible.
a. Reversible: Binding to cholinesterase enzyme is weak (hydrogen bonds) and their actions are easily reversible.
Edrophonium (very short acting, duration of action is around 15 minutes)
Physostigmine, Neostigmine (intermediate acting, duration of action 3-5 hours)
Distigmine (longer acting, duration of action 6-8 hours)
Note: Physostigmine is a natural alkaloid, tertiary amine, more lipid-soluble and can cross blood brain barrier (BBB). Others are synthetic, quaternary amines, less lipid-soluble and poor to cross BBB.
b. Irreversible: Binding to cholinesterase enzyme is strong (covalent bonds) and their actions are not easily reversible. Only few of them are clinically useful and most of them are used as insecticides or war gases. Chemically these are mostly organophosphorous compounds.
Clinically useful: Ecothiophate and Isofluorophate
Insecticides: Alathion and Parathione
War gases: Soman and Tabun
Mechanism: Act indirectly by inhibiting cholinesterase enzyme that metabolizes acetylcholine, thus increase its concentration at the target sites and produce muscarinic and nicotinic actions.
Pharmacological Actions
The pharmacological actions of direct and indirect acting cholinergic drugs are similar and are described together.
A. Muscarinic Actions
a. GI:
They increase the secretion of salivary glands via activation of the muscarinic () receptors. Therefore, Pilocarpine is used in the treatment of dryness of mouth that occurs after radiation therapy for jaw and oral cancer or in Sjogren syndrome (Symptom complex of dry mouth, dry eye, associated with rheumatoid arthritis).
HCl secretion in stomach is increased via activation of receptors on the myenteric neurons and receptors on the parietal cells (Figure 2.2.1).
The exocrine glands and the smooth muscle of GI tract also ha
ve receptors. Their activation increases GI secretion and the peristalsis, while sphincters are relaxed.
These effects permit the use of these drugs in paralytic ileus, e.g. after anaesthesia or abdominal surgery. Toxic doses can cause diarrhoea, intestinal colic and hyperacidity.
(Image Description: A diagram showing the pathway of Vagus nerve stimulation leading to Ach release, acting on receptors of Myenteric neurons, then receptors on Parietal cells and Mast cells. Mast cells release Histamine to receptors, ultimately triggering the Proton Pump (PP) to exchange for .)

Figure 2.2.1. Vagal stimuli, initially in response to smell and taste of food and later presence of food in the stomach, activate neurons of myenteric plexus via receptors. Acetylcholine (Ach) released from these neurons activates receptors on the parietal cells, which in turn trigger ‘Proton pump’ (PP) on the luminal side of the parietal cell to produce HCl. Ach also activates mast cells to release histamine which activates PP to produce HCl via histamine receptors. [Note: PP actively secretes in exchange to . The is passively shifted to the lumen of gastric gland canaliculus to make HCl. In case & ions meet within the parietal cell would burn everything in the cell. The mucosa of the canaliculus is well protected by the mucin and bicarbonate produced by nearby epithelial cells in response to prostaglandin-E (PGE). It may be mentioned here that PG synthesis inhibitors (Aspirin like drugs) reduce this protective role of PGE in the stomach and cause uncontrolled increase in HCl secretion and decrease in mucin and bicarbonate formation leading to hyperacidity, peptic ulceration and bleeding in the stomach (Chapter 4.1, side effects of NSAIDs)].
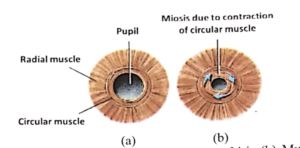
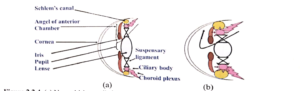
b. Eye: