Adrenergic drugs produce actions like adrenaline and nor-adrenaline in the body and their effects are similar to the stimulation of sympathetic system, therefore, they are also called as sympathomimetic drugs (‘mimic’ means resemble).
Classification
A. Direct acting adrenergic drugs:
These are agonists of adrenergic receptors. According to the chemical structure they are classified as catecholamines and non-catecholamines. Catecholamines have 2 OH groups on benzene ring (at ortho position) and a side-chain, R (Figure 2.4.1).
a. Catecholamines:
Catecholamines include Adrenaline, Noradrenaline and Dopamine. These are present naturally in the body and are also available as synthetic drugs. These are agonists of alpha and beta receptors.
Adrenaline acts on alpha (α1, α2) and beta (β1, β2 and β3) receptors.
Nor-adrenaline acts on α1, α2 and β1 receptors.
Dopamine activates dopamine receptors in addition to its action on α1 and β1-receptors.
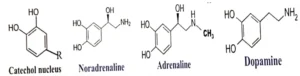
Figure 2.4.1. Structure of catechol nucleus and natural catecholamines in the body.
Catecholamines being less lipid-soluble poorly cross the blood brain barrier and in usual doses have negligible actions on the central nervous system.
b. Non-catecholamines:
These are synthetic compounds and act directly on the adrenergic receptors. According to the specificity of their action on alpha or beta receptors may be further classified as:-
i. Alpha adrenergic drugs:
Selective alpha-1 agonists: Phenylephrine, Naphazoline, Oxymetazoline and Xylometazoline.
Selective alpha-2 agonists: Clonidine and Methyldopa.
ii. Beta adrenergic drugs:
Selective beta-1 agonists, e.g. Dobutamine.
Selective beta-2 agonists e.g. Solbutamol, Terbutaline, Salmeterol and Formoterol.
B. Indirect acting adrenergic drugs:
These drugs increase the concentration of Noradrenaline at the post-ganglionic sympathetic nerve endings, which activates alpha (α1, α2) and beta (β1) receptors at the target sites. They can increase Noradrenaline at the sympathetic nerve endings in two ways:-
i. Increase the release of Noradrenaline, e.g. Tyramine.
ii. Inhibit uptake of Noradrenaline, e.g. Cocaine.
C. Direct & indirect acting adrenergic drugs:
These are agonists of adrenergic receptors and also increase the release of Noradrenaline, e.g. Ephedrine, Pseudoephedrine and Amphetamines. These drugs can activate both alpha (α1, α2) and beta (β1, β2) receptors.
Amphetamines in addition have more prominent central nervous stimulant effects, being more lipid-soluble can easily cross the blood brain barrier.
Mechanism of Action:
Direct acting adrenergic drugs bind to specific adrenergic receptors: Alpha (α), Beta (β), &/or Dopamine (D) receptors. Binding with the receptor causes activation of specific G-proteins: Gs, Gi and Gq proteins. G-proteins in turn stimulate or inhibit adenyl-cyclase or phospholipase-C enzyme and lead to increase or decrease in the formation of 2nd messengers (cAMP/ IP3 & Ca++) and the specific response. The types of adrenergic receptors, G-protein, enzyme and the 2nd messenger involved are given in Table 2.4.1. Interactions of alpha, beta, & D receptor agonists with their receptors, involvement of respective G-proteins and 2nd messengers are depicted in Figures, 2.4. 2-4. The distribution of adrenergic receptors in various body tissues is mentioned in Table 2.4.2.
Table 2.4.1. Adrenergic receptors, types of G-proteins, enzymes and the 2nd messengers.
| Receptor | G-protein | Enzyme | 2nd messenger |
| α1 | Gq | Activate phospholipase-C | Increase IP3& Ca++ |
| α2 | Gi | Inhibit adenyl-cyclase | Decrease cAMP |
| β | Gs | Stimulate adenyl-cyclase | Increase cAMP |
| D1 | Gs | Stimulate adenyl-cyclase | Increase cAMP |
| D2 | Gi | Inhibit adenyl-cyclase | Decrease cAMP |
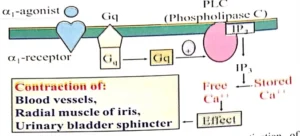
Figure 2.4.2. Interaction of alpha1 agonist, its specific receptos, activation of Gq-protein, Phospholipase-C (PLC), formation of IP3, release of Ca++ and examples of effect produced.,
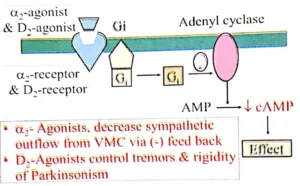
Figure 2.4.3. Interaction of alpha2 and D2 agonists with their specific receptos, activation of Gi-protein, decrease in cAMP formation and examples of effects produced.
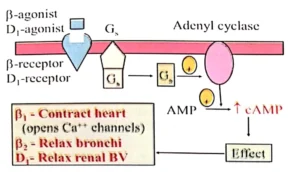
Figure 2.4.4. Interaction of beta (beta1& beta2) agonist with their specific receptos, activation of Gs-protein, increased formation of cAMP and examples of effects produced.
Table 2.4.2. Distribution of adrenergic receptors and the response.
| S. No. | Organ/tissue | Receptor | Response/Action |
| 1. | Heart: | ||
| SA-node | β1 | Tachycardia | |
| AV-node | β1 | Increase conduction | |
| Purkinje system | β1 | Increase conduction | |
| Cardiac muscle | β1 | Increase contraction | |
| Generate ectopic pacemaker | β1 | Arrhythmias | |
| 2. | Blood Vessels | ||
| In skin & splanchnic tissue | α1 | Contraction, increase BP | |
| In skeletal muscle & liver | β2 | Dilatation, lower BP | |
| Coronaries | β2 | Dilatation | |
| 3. | Eye: | ||
| Radial muscle of iris | α1 | Contracts (mydriasis) | |
| Choroid plexus | α2 | Reduce secretions | |
| Intra-occular pressure (IOP) | Lower IOP | ||
| 4. | Respiratory tract: | ||
| Bronchi | β2 | Bronchodilatation | |
| 5. | Kidney: | ||
| J-G cells | β1 | Renin release | |
| 6. | Skin: | ||
| Pilomotor smooth muscle | α1 | Contracts | |
| Sweat glands: Apocrine | α1 | Increase secretion | |
| 7. | Autonomic nerve endings: | ||
| Parasympathetic | α | Reduce acetylcholine release | |
| 8. | Metabolic: | ||
| Liver | β2 | Glycogenolysis, Gluconeogenesis | |
| Fat cells | β3 | Lipolysis | |
| α2 | Inhibit lipolysis | ||
| 9. | Brain: | ||
| Vasomotor center (presynaptic) | α2 | (Rreduce sympathetic outflow from CNS, lower BP & heart rate |
Adrenaline
Adrenaline is synthesized from tyrosine in adrenal medulla and released into bloodstream, along with small quantities of norepinephrine.
Mechanism of action:
Adrenaline is a direct agonist of alpha (alpha1, alpha2) and beta (beta1, beta2,beta3) receptors. Binding with the receptor causes activation of specific G-proteins (Gs, Gi and Gq proteins), depending upon the receptor involved, increased or decreased activity of related enzymes (adenyl-cyclase or phospholipase) and 2nd messengers (cAMP3 & Ca++), leading to the actions, e.g. tachycardia, myocardial contraction, vasoconstriction and bronchodilatation, etc.
Pharmacological actions
CVS:
a. Actions on heart (beta1 receptors): Increased automaticity of SA-node causes tachycardia. Increase in conduction velocity of AV node and purkinje system causes cardiac arrhythmia in overdose. There is also increase in the force of myocardial contraction, cardiac output and blood pressure.
b. Actions on blood vessels: Smooth muscle of blood vessels (BV) in skin, GI and respiratory tract have alpha1 receptors. Vasoconstriction produced in these vessels increases peripheral vascular resistance (PVR) and BP. Coronary arteries, BV in skeletal muscle and liver have beta2$receptors. Vasodilatation produced increases blood flow to these sites.
c. Action on BP: Systolic BP is increased due to increase of peripheral vascular resistance (vasoconstriction), CO (myocardial contraction), and heart rate. Diastolic BP may be slightly decreased due to vasodilatation in some vascular beds, like BV in the skeletal muscle and liver. The biphasic action of adrenaline can be demonstrated in experimental animals by an IV injection of adrenaline and then IV phenoxybenzamine (to block alpha1 mediated vasoconstriction) before IV injection of adrenaline (Figure 2.4.5).
![Waveform graph showing Adrenaline injection effect and Phenoxybenzamine before Adrenaline effect]
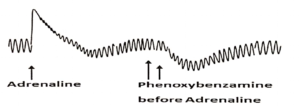
Figure 2.4.5. Adrenaline injection initially causes sudden rise in BP due to $\alpha_1$-mediated vasoconstriction, which gradually comes to normal and is followed by some decrease in BP due to (beta2-mediated vasodilatation. When an alpha1-blocker (phenoxybenzamine) is given before adrenaline there is no alpha1-mediated rise in BP, but there is a more profound fall in BP due to beta2-mediated vasodilatation (called as ‘Vaso-reversal phenomenon of Dale’).
Kidneys:
Renin released from JG-cells in kidney converts angiotensinogen to angiotensin-I, which is then changed to angiotensin-II by Angiotensin Converting Enzyme (ACE). Angiotensin-II is a potent vasoconstrictor and increases BP. Angiotensin II also increases release of aldosterone from the adrenal cortex, which increases Na and water reabsorption from the kidneys, blood volume and BP.
Actions on smooth muscle:
Adrenaline relaxes bronchial smooth muscle (beta2-mediated bronchodilatation), and thus relieves bronchospasm of asthma and allergic conditions. Also relaxes uterine smooth muscle and can prevent premature labour. Relaxation of longitudinal smooth muscle of GI and constriction of circular muscle of sphincters cause constipation. Relaxation of urinary bladder wall and constriction of bladder sphincter may result to urine retention.
However, some smooth muscles contract, due to presence of alpha1-receptors, like radial muscle of iris (produce mydriasis), smooth muscle of seminal vesicles (causes ejaculation) and pilomotor muscle in hair follicle (Piloerection or ‘goose skin’).
Sweat glands:
Excess adrenaline released during anxiety increases secretions of apocrine sweat glands in palms, soles, and armpits.
Metabolic effects:
a. Hyperglycemia is produced due to increased glycogenolysis and gluconeogenesis in liver, increased release of glucagon from alpha-cells of pancreas and decreased release of insulin from beta-cells of pancreas.
b. Free fatty acids in plasma are increased due to lipolysis.
CNS:
Adrenaline and other catecholamines are poorly-lipid soluble and difficult to cross blood brain barrier. However, in overdosage can cause confusion, restlessness and tremors
Uses:
Hypersensitivity reactions (due to drugs and pollens, etc.): dermatitis, angiodema, hypotension and anaphylactic shock
Cardiac arrest
As local haemostatic (to stop bleeding), e.g. after tooth extraction
To prolong the effect of local anaesthetics
Acute severe asthma
Open angle glaucoma
Adverse effects:
In usual doses there may be tachycardia, palpitation, cold extremeties and headache.
In bit higher doses can produce ectopic beats, atrial and ventricular arrhythmias, hypertension, angina and cerebral stroke.
Overdosage ia also associated with anxiety, tremors, confusion, restlessness, hyperglycemia and hyperlipidemia.
Nor-Adrenaline
It possesses alpha (alpha1 and alpha2) and beta (beta1) agonistic effects but lacks beta2-effefcts.
Uses:
It is used for the treatment of hypotension caused by the anesthetic agents. It may be given along with local anesthetics to prolong their dduration of action.
Adverse effects:
It can cause hypertension and cardiac arrhythmias in high doses.
Dopamine
Besides action on dopamine receptors it possesses alpha (alpha1) and beta (beta1) agonistic effects. It is preferred for the treatment of hypotension and shock as it prevents renal ischemia because it can dilate renal blood vessels due to the presence of D1 receptors in these vesels.
Selective alpha-1 (alpha1) adrenergic drugs
Phenylephrine, Oxymetazoline and Xylometazoline, etc.
These drugs act mainly as direct agonists on alpha1-receptors and produce actions similar to adrenaline at different sites having $\alpha_1$-receptors, like vasoconstriction, pupil dilatation (mydriasis) and the relaxation of the smooth muscle of intestines.
Uses:
a. They are mainly used for the relief of nasal and sinus congestion (decongestant) and are available over the counter in combnination with a non-opioid analgesic (e.g. Paracetamol and Aspirin).
b. Phenylephrine is available as eye drops and frequently used for the ophthalmic examination.
c. In combination with local anesthetics they are employed to increase the duration of action of local anesthetic agents in dental practice.
Adverse Effects:
In the doses used for the relief of nasal congestion or along with local anesthetic they are quite safe. However, in overdose, e.g. repeated injections for local anesthesia, they may cause headache, anxiety, tremors, tachycardia, palpitation and mild increase in blood pressure. Therefore, should be given carefully in patients with hypertension.
Selective alpha-2 (alpha2) adrenergic drugs
Methyldopa and Clonidine.
These drugs reduce the sympathetic outflow from the CNS by the stimulation of pre-synaptic $\alpha_2$-receptors in the vasomotor center (VMC) in the midbrain, can lower blood pressure and heart rate and are used in the treatment of hypertension. They are discussed in Chapter 2.5 and also along with anyihypertensive drugs in Volume II.
Selective beta-1 (beta1) adrenergic agonists
Dobutamine
Increases heart rate and BP and is used in acute heart failure. It has been dicussed in detail along with other drugs for the treatment of heart failure in Volume II.
Selective beta-2 (beta2) adrenergic agonists
Salbutamol and Terbutaline, etc.
They produce bronchodilatation and are used in asthma and chronic obstructive pulmonary disease (COPD). They are dicussed in detail along with other drugs for asthma and COPD in Volume II.
Oral and Dental Implications of Adrenergic Drugs
a. Local anesthetics are commonly used in dentistry in combination with a vasoconstrictors (e.g. adrenaline, noradrenalne, phenylephrine and levonordefrin) to prolong the duration of local anesthesia. Excessive use of such combination may lead to tachycardia and hypertension. Reports of serious outcomes with local anesthetic-vasoconstrictor use are very rare. Reason being that, adrenaline is more commonly used for this purpose, which has alpha-1adrenergic effects on most vascular beds, leading to vasoconstriction, as well as beta-2 adrenergic effects on some other vascular beds, e.g. BV in skeletal muscle resulting in vasodilatation (Figure 2.4.2). This opposing vasodilatation limits the potential pressor effects of adrenaline compared to other vasoconstrictors, like Noradrenaline and Phenylephrine, etc.
b. Nonselective beta-adrenergic blocking agents (e.g. Propranolol) are used in the treatment of hypertension and angina. If a patient is taking a nonselective beta-blocker and is given local anesthetic with Adrenaline, the beta-2 vasodilatory effects (and the beta-1 cardiac stimulatory effects) of Epinephrine will be blocked and unopposed alpha-1 vasoconstriction would increase the blood pressure. Such interaction is less likely to occur with cardio-selective beta-blocking agents, like Atenolol, and Metoprolol, etc. Patients with cardiovascular disease are particularly vulnerable to the pressor effects of the combination of vasoconstrictor with local anesthetic.
c. Patients with asthma and COPD are often treated with beta 2-adrenergic agonists. These drugs can cause alternations in the amount and proetein contents of salivary glands secretions, resulting in a decrease in the protective function of saliva on the teeth.
d. Tricyclic antidepressant (e.g. Imipramine, Amitriptyline and Nortriptyline) block noradrenergic reuptake pump. Patients taking these drugs are more likely to get tachycardia and hypertension with dental vasoconstrictors. Selective serotonin reuptake inhibitors block the serotonin reuptake therefore, are not associated with adverse drug interactions with dental vasoconstrictors.
e. Like tricyclic antidepressant, Cocaine also inhibits catecholamine reuptake at adrenergic nerve endings, may also enhance vasoconstrictor effect of dental vasoconstrictors. A number of deaths have been attributed to interaction between dental vasoconstrictors and Cocaine abuse.