Antiadrenergic drugs block the actions produced by noradrenaline released at the post-ganglionic sympathetic nerve endings and adrenaline and noradrenaline produced by the adrenal medulla. In other words they counter the effects produced by sympathetic stimulation and thus are also named as sympatholytic drugs. They also block the actions of exogenous sympathomimetic compounds on their corresponding receptors.
Classification
They can be classified according to the type of adrenergic receptors they can block and according to the inhibition of the synthesis and the release of adrenergic neurotransmitter; such as:- I. Alpha adrenergic blockers II. Beta adrenergic blockers III. Adrenergic neuron blockers IV. Presynaptic alpha-2 agonists
I. Alpha adrenergic blockers
Alpha-adrenergic blocking drugs may be sub-classified as: A. Selective block alpha-1 – receptor blockers B. Selective alpha-1A – receptor blockers C. Non-selective alpha– blockers, i.e. block both alpha-1 and alpha-2 – receptors.
A. Selective alpha-1- adrenergic blockers,
e.g. Prazosin, Terazosin and Doxazosin
Mechanism of action: These drugs competitively blocks alpha-1-receptors in the target sites. Thus inhibit the actions of endogenous catecholamine as well as block the actions of sympathomimetic drugs on alpha-1-receptors.
Pharmacological actions
CVS: Blockade of alpha-1-receptors in the blood vessels causes vasodilatation, decrease in peripheral vascular resistance and hypotension. Low blood pressure causes reflex tachycardia. Blockade of alpha-1-receptors in the blood vessels also causes orthostatic hypotension (or postural hypotension). Which means, when a person in sitting for some time, e.g. on a dental chair, there is pooling of blood in the peripheral vessels in the lower extremities. This pooling of blood is further increased because of vasodilatation caused by the alpha blocking drug.
When the patient suddenly gets up after completion of the dental treatment, feels dizzy, lethargic, may vomit and fall down (Syncopal attack), due to low blood pressure and poor blood flow to brain. Normally, alpha-1-receptor mediated reflex peripheral vasoconstriction immediately compensates and ensures enough blood perfusion to vital organs, including brain. But in a patient taking alpha blocking drug this compensatory reflex is obtunded. Therefore, a person taking alpha-adrenergic receptor blocker or a vasodilator, e.g. for the treatment of his/her blood pressure, should be advised to get up very slowly from the dental chair after the treatment.
Upper respiratory tract: Dilatation of blood vessels in the nose causes nasal congestion.
GI:
Blockade of alpha-1-receptors in the GI tract results into parasympathetic over activity and increased gastro-intestinal motility and secretions, including hyperacidity.
GU:
Blockade of alpha-1A– & alpha-1D receptors in the smooth muscle of prostate and bladder neck causes their relaxation and a decrease in resistance to urine flow. [Note: Resistance to urine flow is increased in benign prostatic hypertrophy (BPH)]. Also inhibit ejaculation, which may be troublesome for some and useful for those suffering from premature ejaculation.
Prazosin is relatively short acting (Plasma half-life, 3-4 hours) and Terazosin and Doxazosin are a bit longer acting (Plasma half-lives, 9-12 hours and 22 hours, respectively).
Uses:
a. The alpha blocking drugs have been commonly used for the treatment of hypertension in the past, but currently are rarely employed because of the availability of safer drugs, e.g. angiotensin inhibitors, angiotensin receptor blockers and calcium channel blockers.
b. They are used in the Raynaud’s phenomenon (peripheral vasoconstriction in subcutaneous tissue of finger and toes in response to cold).
c. They are frequently used for the relief of obstruction to urine flow in the BPH, particularly more selective alpha-1A– adrenergic blockers.
B. Selective alpha-1A– adrenergic blockers,
e.g. Tamsulosin and Alfuzosin.
Mechanism of action: Tamsulosin and Alfuzosin are more selective for alpha-1A– & 1D receptor subtypes, which are present in the smooth muscle of prostate and bladder neck. Their blockade causes relaxation of smooth muscle of prostate and bladder neck, easing urine flow.
Uses:
They are commonly used for the management of bladder outlet obstruction (BOO), due to BPH. They lack effect on blood pressure as compared to other alpha blockers. Tamsulosin is longer acting and can be administered once-daily. [Note: Other alpha blockers, e.g. Doxazosin may also be used for the management of BOO in hypertensive patients].
C. Non-selective alpha-adrenergic blocking drugs,
e.g. Phenoxybenzamine and Phentolamine.
Mechanism of action: These drugs competitively block alpha-1 receptors in the smooth muscle of blood vessels and cause vasodilatation, reduce peripheral resistance and lower the blood pressure. Also can block presynaptic alpha-2 receptors in the vasomotor center (VMC) in the midbrain and tend to increase the sympathetic out-flow from the brain and increase the blood pressure and heart rate. But the peripheral effects are more dominant.
Phenoxybenzamine irreversibly blocks the actions of catecholamines (Noradrenaline, Adrenaline and Dopamine) on both the alpha-1 and alpha-2-receptors, therefore, it is longer acting. Its plasma half-life is around 24 hours. Whereas, blockade of these receptors with Phentolamine is reversible and shorter acting, with an half-life of 1-2 hours.
Uses:
Phenoxybenzamine is mainly used in the management of Pheochromocytoma, which is a tumor of the chromaffin tissue of the adrenal gland, secretes catecholamines and causes sever hypertension. When the tumor is solitary and removable, best treatment is surgery. Then Phenoxybenzamine is given before surgery while waiting for operation.
Phentolamine is usually given at the time of operation to counter the effect of catecholamines released during the surgical maneuver. A beta-blocker, like Atenolol, is also given to block the beta-effects of the catecholamines released, particularly on beta-1-receptors in the heart. When tumors are multiple, small, scattered, and difficult to operate, then Phenoxybenzamine and a beta blocker are used for the management of pheochromocytoma.
Adverse effects of alpha-blockers (Selective & non-selective):
Both the non-selective and alpha-1-selective alpha blockers can cause:
a. Miosis. This is due to unopposed contraction of the circular muscle of iris when the radial muscle is relaxed due to blockade of alpha-1 receptors in the radial muscle.
b. Nasal and sinus congestion occurs due to vasodilatation in upper respiratory tract.
c. Orthostatic (or postural) hypotension. When the patient suddenly gets up from the sitting or lying position (e.g. from the dental chair), there is pooling of blood in the lower extremities due to gravity, which is increased due to vasodilatation with alpha blockers. The blood pressure falls down and there is poor blood supply to the upper part of the body including brain. Which results in dizziness, fainting, tachycardia, vomiting and lethargy. Normal compensatory reflexes fail to cause vasoconstriction and maintain the blood pressure as alpha-1-receptors in the blood vessels are blocked. Therefore, patient using alpha blockers should get up slowly from the dental chair.
e. Unopposed cholinergic effects: Hyperacidity, peptic ulcer, diarrhea and intestinal colic can occur due to unopposed cholinergic effects when alpha-1-adrenergic effects are blocked in GI.
II. Beta adrenergic blockers
A. Cardio-non-selective beta blockers (Mixed beta-1 and beta-2-blockers)
B. Cardio-selective beta blockers (Selective beta-1-blockers)
C. Beta blockers with intrinsic sympathetic activity
D. Beta blockers used topically in eye
E. Alpha and beta blockers
Mechanism of action:
Beta-blockers competitively block the actions of sympathetic transmitter Noradrenaline and Adrenaline on the beta-adrenergic receptors (or simply beta-receptors), as well as the actions of beta-adrenergic agonists.
Pharmacological actions and uses:
a. CVS:
The major clinically useful cardiovascular effects of Beta-blockers include: Antihypertensive, antianginal and antiarrhythmic.
Antihypertensive: They lower blood pressure by blocking beta-1-receptors in the heart and Juxtaglomerular cells (JG-cels) in the kidneys.
Beta-1-blockade in the heart: (SA-node and myocardium) decreases the heart rate, force of myocardial contraction and the cardiac out-put, thus lower the blood pressure.
Beta-1-blockade in the kidneys: decreases renin release which in turn decreases angiotensin formation. The decrease in angiotensin causes vasodilatation and a decrease in the sodium and water retention by the kidneys (via decrease in the release of aldosterone from the adrenal cortex). Vasodilatation decreases peripheral vascular resistance, while decrease of Na & water retension lowers blood volume and venous return. Together these effects lower BP.
Antianginal: They relieve angina by decreasing the force of myocardial contraction by blocking beta-1-receptors in the heart muscle, thus reduce the oxygen demand of the myocardium. Decrease in peripheral vascular resistance and venous return, mentioned above, lower the work load on heart. Together these effects relieve and prevent angina.
Antiarrhythmic: They are particularly useful in Paroxysmal Supraventricular Tachycardia. They reduce the heart rate and atrioventricular conduction by blocking beta-1-receptors in SA-node, AV-node and purkinje fibers. Thus ventricular rate is controlled and cardiac output is improved.
b. Other actions and uses:
i. Hyperthyroidism: Thyroid hormones sensitize adrenergic receptor to the action of natural catecholamines (Adrenaline and Noradrenaline) and produce symptoms of sympathetic overactivity, i.e. tachycardia, palpitations, insomnia, anxiety and tension. Propranolol, being more lipid soluble and easy to cross the blood brain barrier is commonly used to control sympathetic over activity associated with hyperthyroidism. Propranolol effectively controls both the cardiovascular and the central nervous symptoms of hyperthyroidism.
ii. Glaucoma: Reduce the formation of aqueous humour. Timolol and Betaxolol are available as eye drops and are used topically for the treatment of open-angle glaucoma.
Relieve sympathetic over activity related to anxiety and tension and also useful in the prophylaxis of migraine. Propranolol, which is highly lipid soluble and easily crosses blood brain barrier, is more commonly used for this purpose.
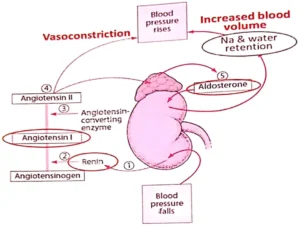
Figure 2.5.1. Renin-Angiotensin-Aldosterone system. In response to low blood pressure (bottom), renin is released from JG-cells in the kidney (1), converts angiotensinogen to angiotensin-I, which is changed to angiotensin-II by angiotensin converting enzyme (ACE) (2 & 3). Angiotensin-II causes vasoconstriction (4) and aldosterone secretion from the supra-renal gland (5). Aldosterone retains Na and water from renal tubules and increases blood volume. Vasoconstriction and increase in blood volume increases blood pressure (top).
A. Cardio-non-selective beta blockers:
e.g. Propranolol, Nadolol and Esmolol, etc.
Propranolol was the first beta-blocker introduced and is considered as the prototype drug amongst the group. Still easily available and commonly used. Propranolol and Nadolol are primarily used for the treatment of essential hypertension, portal hypertension, angina and cardiac arrhythmia. Propranolol is used to control sympathetic over activity associated with hyperthyroidism. Propranolol is also effective in the treatment of anxiety and migraine.
Non-selective beta blockers may have some problems due to beta-2-receptor blockade in some tissues, i.e. bronchospasm, hypoglycemia and constriction of blood vessels in the skeletal muscle:-
Bronchospasm occurs because of unopposed constriction of bronchi with parasympathetic supply when beta-2-receptor (sympathetic) are blocked.
Hypoglycemia is due to inhibition of beta-2-receptor mediated glycogenolysis and gluconeogenesis in the liver. Thus may require adjustment of dose of hypoglycemic drugs in diabetic patients.
These problems are negligible in normal individuals. However, non-selective beta blockers should be avoided in patients of asthma, diabetes and peripheral vascular disease.
Esmolol is the shortest acting beta blocker and used for the treatment of hypertensive emergency and supraventricular tachycardia. Once blood pressure or arrhythmia is controlled with Esmolol, is maintained with other drugs.
Nadolol is longer acting and is used for the maintenance therapy in portal hypertension.
B. Cardio-selective beta blockers:
e.g. Atenolol and Metoprolol, etc. Atenolol is more frequently used for the treatment of hypertension and angina. Possesses minimal beta-2-receptor mediated side effects, i.e. bronchospasm, hypoglycemia and muscle pain and fatigue. It is also less lipid soluble, poor to cross blood brain barrier and has little central nervous side effects. Metoprolol is more lipid soluble and can cause central nervous side effects, which are given below.
C. Beta blockers with intrinsic sympathetic activity:
e.g. Acebutolol and Pindolol, etc. These drugs have partial agonistic activity in overdosage and are used for hypertension and arrhythmia. If required, can be given in a bit higher dose with minimum cardiac depression. Because, when the dose is increased their sympathetic activity ensues and avoids cardiac depression.
D. Beta blockers used topically in glaucoma:
e.g. Timolol and Betaxolol, etc. These are available as eye drops and commonly used topically for the management of open angle glaucoma, as they decrease the formation of aqueous humor.
E. Alpha and beta blockers:
e.g. Labetalol and Carvedilol, etc. Block both alpha and beta receptors. Blockade of alpha-1 receptors dilates blood vessels and lowers blood pressure. While block of beta-1 receptors decreases heart rate, CO, and BP. However, beta-2 receptors block causes bronchospasm, hypoglycemia and muscle pain and fatigue. Labetalol is a useful alternate to methyldopa in hypertension during pregnancy. Labetalol is given IV in hypertensive emergency. Labetalol and Carvedilol can also be used in the treatment of heart failure, particularly when symptoms due to compensatory sympathetic over activity are more marked and troublesome, e.g. tachycardia, palpitation and cold extremities due to vasoconstriction.
Adverse effects of Beta-Blockers:
Cardiac: In higher doses, these drugs can cause bradycardia, hypotension, and heart failure. Drugs with intrinsic sympathetic activity, such as Pindolol, are less likely to lead to heart failure.
Respiratory: Blockade of beta-2 receptors in the bronchi leads to unopposed cholinergic effects, causing bronchoconstriction. While cardio-selective beta blockers cause fewer bronchial problems, all beta blockers should generally be avoided in asthmatic patients.
Metabolic: Blockade of beta-2 receptors in the liver decreases glycogenolysis, producing hypoglycemia. This can potentiate the effects of hypoglycemic drugs in diabetic patients. Furthermore, beta blockers mask the warning signs of hypoglycemia (tachycardia, palpitations, and sweating), which can be life-threatening.
CNS: Depression and nightmares are commonly reported. Highly lipid-soluble blockers like Propranolol and Metoprolol cross the blood-brain barrier easily and are more prone to these side effects.
Fatigue and muscle pains: This results from reduced blood supply to skeletal muscles. When beta-2 receptors (which normally cause vasodilatation) are blocked, unopposed alpha-1 activation constricts blood vessels, leading to ischemic pain and fatigue.
Cold extremities: Blockade of beta-2 receptors in skin blood vessels allows unopposed alpha effects to cause vasoconstriction, reducing blood flow to the extremities.
III. Adrenergic Neuron Blockers:
e.g. Reserpine and Guanethidine.
a. Reserpine:
Reserpine is an alkaloid from Rauwolfia serpentina (Snake root), native to the Indian Subcontinent. Historically used in folk medicine for insanity, it was originally isolated by Prof. Dr. Attaullah (Karachi University) and named Ajmaline, later named Reserpine by German scientists.
Mechanism of action: Reserpine blocks the uptake of serotonin, norepinephrine, and dopamine into presynaptic storage vesicles by inhibiting Vesicular Mono-Amine Transporter-2 (VMAT-2) in the adrenergic neuron terminal. The monoamines remaining in the cytoplasm are metabolized by the monoamine oxidase (MAO) enzyme, leading to the depletion of these neurotransmitters in both peripheral and central nerve terminals.
Antihypertensive effect: The depletion of Noradrenaline in peripheral sympathetic neurons decreases peripheral vascular resistance, cardiac contraction, and cardiac output, thereby lowering blood pressure.
Dopamine depletion: The depletion of Dopamine in the central neurons particularly in the limbic system is perhaps associated with its beneficial effect in Schizophrenia. Because Dopamine () receptor antagonists are effective antipsychotics drugs.
Uses: Reserpine has been used for the treatment of mild to moderate hypertension. Its behavioral effects reported in the folk medicine for the treatment of insanity can be related to the depletion of dopamine in the dopaminergic neurons in the limbic system. Currently, its use has declined due to availability of safer drugs both for hypertension and schizophrenia.
b. Guanethidine:
A synthetic drug, designed to reduce sympathetic activity. Mechanism of action: It is taken up by the adrenergic neurons by Norepinephrine Transporter (NET) and replaces noradrenaline in the storage vesicles of the adrenergic nerve terminals. Thus reduces stores and release of adrenergic transmitter and lowers the blood pressure (Figure 2.5.2b).
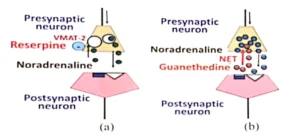
Figure 2.5.2. (a) Reserpine blocks uptake of norepinephrine and amines into presynaptic storage vesicles by blocking Vesicular Mono-Amine Transporter-2 (VMAT-2) in the adrenergic neuron terminal (b) Guanethidine is taken up by the adrenergic neurons by Nor-Epinephrine Transporter (NET) and replaces noradrenaline in the storage vesicles of presynaptic adrenergic nerve terminal.
Uses: Guanethidine have been commonly used in the past for the treatment of mild to moderate hypertension. Its use has declined due to availability of safer antihypertensive agents. However, Guanethedine is still licensed in the UK and some other countries. It is also available as eye drops for treatment of open angle glaucoma, as it reduces aqueous humor formation.
IV. Presynaptic Alpha-2 Agonists (Central sympatholytics):
e.g. Methyldopa and Clonidine Mechanism of action: Methyldopa is converted in the body to an active metabolite (a-methyl-noradrenaline). Clonidine is itself active. Both stimulate pre-synaptic alpha-2 receptors in VMC. They decrease Noradrenaline release from neurons of VMC, thus decrease sympathetic outflow from CNS and decrease heart rate, CO, PVR & BP (Figure 2.5.3).
Uses: Methyldopa: Because of the known safety of methyldopa in pregnancy, it is commonly used for the treatment of hypertension during pregnancy. Clonidine: It is used to control the withdrawal symptoms of alcohol and other drugs of abuse. It is also advised for the treatment of attention deficit hyperactivity disorder (ADHD).
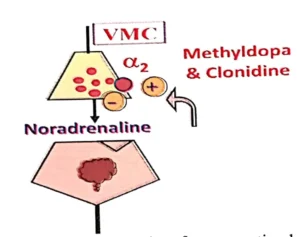
Figurfe 2.5.3. Methyldopa and Clonidine are agonist of presynaptic alpha-2 receptors and reduce the release of Noradrenaline from the nerve terminals in the Vaso Motor Center (VMC). Thus decrease sympathetic outflow from the CNS and decrease heart rate, CO, PVR & BP.
Adverse Effects: Methyldopa: Nightmares, mental depression, extrapyramidal effects and lactation Clonidine: Dry mouth, sedation, mental depression and rebound increase in BP when stopped.