Fungal infections, medically termed mycoses, range from superficial skin diseases to life-threatening systemic infections. Unlike bacteria, fungi are eukaryotic organisms with a rigid cell wall composed primarily of chitin and a plasma membrane containing ergosterol instead of cholesterol. These structural differences form the foundation of antifungal pharmacology.
Over the past few decades, the incidence of invasive fungal infections—such as candidemia and cryptococcosis—has increased significantly. This rise is largely attributed to:
Organ transplantation
Cancer chemotherapy
Long-term corticosteroid use
HIV/AIDS
Advanced critical care interventions
Effective antifungal therapy requires understanding both fungal biology and drug mechanisms.
Major Targets of Antifungal Drugs
Antifungal drugs act by targeting:
Ergosterol in the fungal cell membrane
Ergosterol synthesis pathways
β(1,3)-D-glucan synthesis in the fungal cell wall
DNA/RNA synthesis
Mitotic spindle formation
These targets allow selective toxicity while minimizing damage to human cells.
Drugs for Subcutaneous and Systemic Mycotic Infections
Systemic mycoses require aggressive and often prolonged therapy. The following drug classes form the backbone of treatment.
1. Amphotericin B (Polyene Antifungal)
Amphotericin B remains one of the most potent antifungal agents available and is often reserved for severe, life-threatening infections.
Mechanism of Action
Binds directly to ergosterol
Forms membrane pores
Causes leakage of potassium and intracellular components
Results in fungal cell death
It is generally fungicidal.
Spectrum of Activity
Active against:
Candida albicans
Cryptococcus neoformans
Histoplasma capsulatum
Blastomyces dermatitidis
Coccidioides immitis
Many strains of Aspergillus
Also used in leishmaniasis.
Pharmacokinetics
Administered via slow IV infusion
Highly protein bound
Poor CSF penetration (improves with inflammation)
Liposomal formulations reduce renal toxicity
Adverse Effects (High-Yield)
Nephrotoxicity (most significant)
Fever and chills (infusion reactions)
Hypokalemia
Hypotension
Anemia
Despite toxicity, it remains a drug of choice in severe fungal infections.
2. Flucytosine (5-FC)
Flucytosine is a synthetic antimetabolite often used in combination therapy.
Mechanism of Action
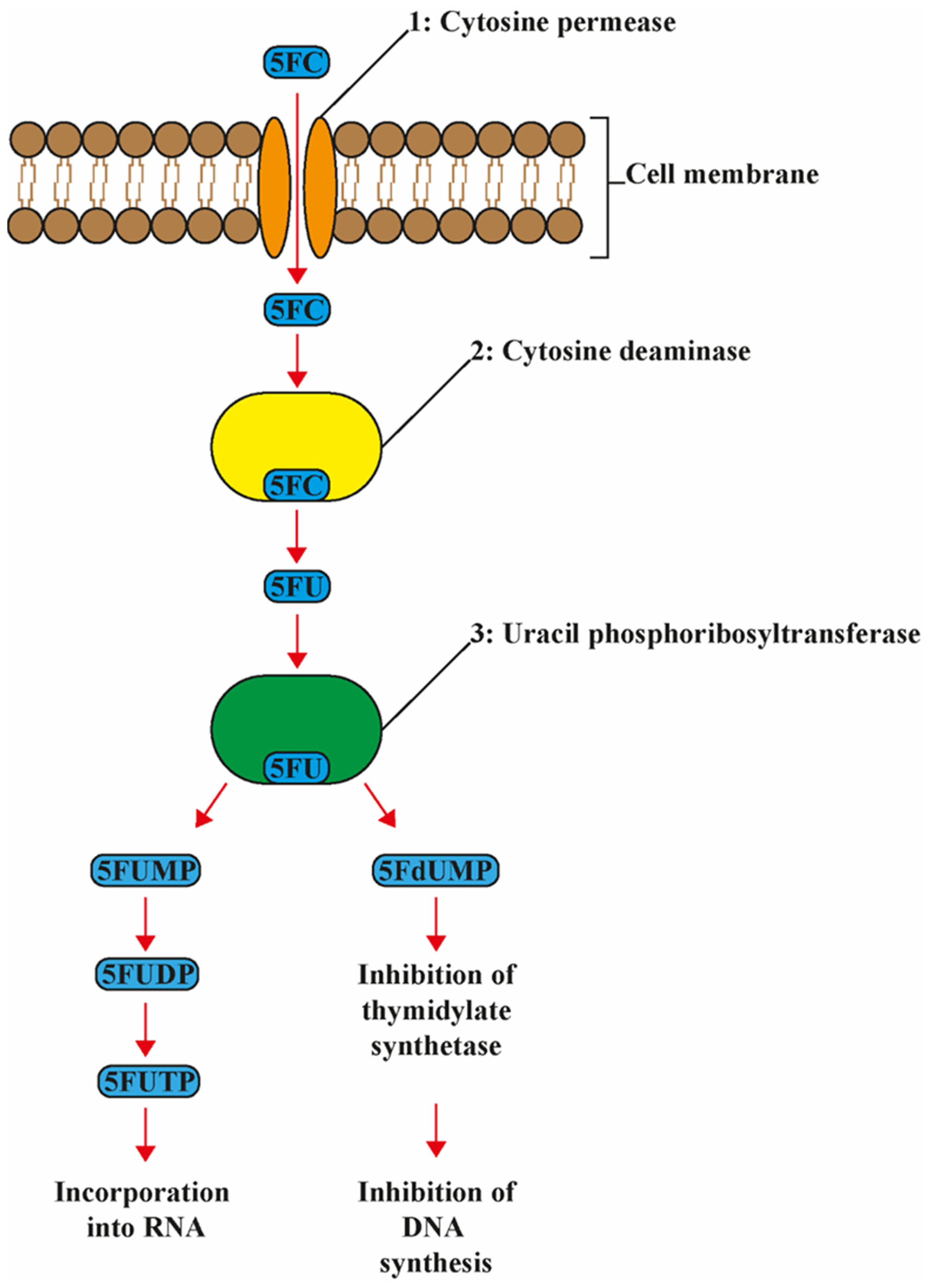

Enters fungal cells via cytosine permease
Converted to 5-fluorouracil
Inhibits DNA and RNA synthesis
It is fungistatic and commonly combined with amphotericin B to reduce resistance.
Clinical Uses
Cryptococcal meningitis
Severe candidiasis
Adverse Effects
Bone marrow suppression
Neutropenia
Thrombocytopenia
Hepatotoxicity
GI disturbances
Dose adjustment is required in renal impairment.
3. Azole Antifungals
Azoles are among the most widely used antifungal agents and are divided into imidazoles (topical) and triazoles (systemic).
Mechanism of Action

Inhibit C-14 α-demethylase (CYP450 enzyme)
Block conversion of lanosterol to ergosterol
Disrupt membrane integrity
Mostly fungistatic
Drug Interactions
Azoles inhibit hepatic CYP450 enzymes, leading to significant drug interactions.
A. Fluconazole
Excellent oral bioavailability
Penetrates CSF
Drug of choice for cryptococcal meningitis maintenance
Used in candidiasis and coccidioidomycosis
Adverse effects:
Nausea
Rash
Hepatotoxicity
B. Itraconazole
Broader spectrum than fluconazole.
Indications:
Histoplasmosis
Blastomycosis
Sporotrichosis
Important caution:
Negative inotropic effect (avoid in heart failure)
C. Voriconazole
Drug of choice for invasive aspergillosis
Excellent tissue penetration
Nonlinear pharmacokinetics
Unique adverse effects:
Visual disturbances
Hallucinations
Hepatotoxicity
D. Posaconazole
Broad-spectrum coverage
Used in immunocompromised patients
Strong CYP3A4 inhibitor
Effective for resistant fungal infections
4. Echinocandins
Examples:
Caspofungin
Micafungin
Anidulafungin
Mechanism of Action
Inhibit β(1,3)-D-glucan synthesis
Disrupt fungal cell wall
Fungicidal against Candida
Clinical Uses
Invasive candidiasis
Candidemia
Alternative therapy for aspergillosis
Adverse Effects
Fever
Rash
Infusion-related reactions
Generally well tolerated compared to amphotericin B.
Drugs for Cutaneous Mycotic Infections
Cutaneous infections (dermatophytes) affect skin, hair, and nails.
Common organisms:
Trichophyton
Microsporum
Epidermophyton
1. Terbinafine (Squalene Epoxidase Inhibitor)
Mechanism

Inhibits squalene epoxidase
Blocks ergosterol synthesis
Causes toxic squalene accumulation
Drug of choice for:
Onychomycosis
Tinea capitis
Adverse effects:
GI upset
Taste disturbance
Hepatotoxicity
2. Griseofulvin
Inhibits mitotic spindle formation
Fungistatic
Requires prolonged therapy
Induces hepatic CYP450 enzymes
Used for scalp and hair dermatophyte infections.
3. Nystatin
Polyene similar to amphotericin B
Used for:
Oral candidiasis
Vaginal candidiasis
Cutaneous candidiasis
Not absorbed systemically
4. Topical Imidazoles
Examples:
Clotrimazole
Miconazole
Ketoconazole (topical)
Used for:
Tinea pedis
Tinea corporis
Vulvovaginal candidiasis
Oropharyngeal candidiasis
High-Yield Clinical Correlations
HIV patient with cryptococcal meningitis → Amphotericin B + Flucytosine
Invasive aspergillosis → Voriconazole
Nail fungal infection → Oral Terbinafine
Oral thrush → Nystatin
Candidemia → Echinocandins
Conclusion
Antifungal pharmacology centers on selective targeting of ergosterol and fungal cell wall components. While effective, many systemic antifungal drugs carry significant toxicity and drug interaction risks.
Choosing the appropriate antifungal therapy requires consideration of:
Type of organism
Site of infection
Immune status
Drug toxicity profile
Potential drug interactions
A strong understanding of mechanisms, spectrum, pharmacokinetics, and adverse effects is essential for safe and effective management of fungal infections.