Introduction
Anticholinergic drugs can antagonize the actions of acetylcholine and other cholinergic drugs. Acetylcholine and cholinergic drugs have two types of actions, muscarinic and nicotinic, mediated by muscarinic and nicotinic receptors on the target sites. Some anticholinergic drugs more specifically block muscarinic receptors and others block nicotinic receptors. Therefore, anticholinergic drugs may be classified as Anti-muscarinic and Anti-nicotinic drugs.
The muscarinic receptors are mainly distributed at the post-ganglionic parasympathetic neurons, Therefore, antimuscarinic drugs produce actions similar to parasympathetic block and may also be called as ‘Parasympatholytic Drugs’ and are discussed in this chapter.
Whereas, the nicotinic receptors are present in the autonomic ganglia and the neuromuscular junction of the skeletal muscle. Therefore, the anti-nicotinic drugs may be sub-grouped into the ‘Ganglionic Blockers’ and the ‘Neuromuscular Junction Blockers’ and are described in Chapter 2.6 and 6.6, respectively.
Anti-muscarinic drugs (Parasympatholytic drugs)
Mechanism of action:
These drugs competitively block muscarinic receptors. As the muscarinic receptors are present at the target sites supplied by the post-ganglionic parasympathetic nerves, therefore, antimuscarinic drugs antagonize actions of acetylcholine or cholinergic drugs on these sites.
Classification:
According to the chemical structure and some specific properties related to the structure, antimuscarinic drugs can be divided into two sub-groups:
I. Tertiary amines:
a. Natural alkaloids: e.g. Atropine and Hyoscine (Scopolamine)
b. Synthetic compounds: i) for intestinal and ureteric colic: Dicyclomine and Difemerine, etc.
ii) for Parkinsonism: Benztropine and Procyclidine, etc.
II. Quaternary amines:
These are synthetic compounds; a) for peptic ulcer: Pirenzepine; ii) for asthma: Ipratropium and Tiatropium; iii) for intestinal and ureteric colic: Hyoscine-N-butyl bromide, Propantheline and Glycopyrrolate, etc.
[Note: The tertiary amines are more lipid-soluble and easy to cross the blood brain barrier (BBB). So besides peripheral effects also possess the central nervous effects. The quaternary amines are less-lipid soluble, difficult to cross BBB and have negligible actions on the central nervous system].
Pharmacological actions
GI:
a. They block muscarinic M3 receptors on the exocrine glands. Thus decrease the secretions of the salivary glands and can cause dryness of mouth. Intestinal secretions are also reduced, which contribute to constipation.
b. Block muscarinic M1 receptors on the neurons supplying the parietal cells and decrease the gastric HCl secretion.
c. Block muscarinic M3 receptors on the smooth muscle of GI; decrease peristalsis, constrict the sphincters and cause constipation.
Eye:
Block M3 receptors on circular muscle of iris, ciliary body and lacrimal glands, and cause:-
a. Mydriasis (dilatation of pupil). This is due to the relaxation of circular muscle and unopposed contraction of radial muscle of iris (Figure 2.3.1)
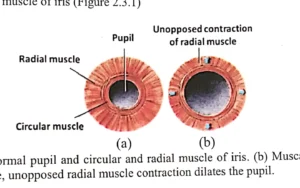
Figure 2.3.1. (a) Normal pupil and circular and radial muscle of iris. (b) Muscarinic antagonists relax circular muscle, unopposed radial muscle contraction dilates the pupil.
b. Cycloplegia (loss of accomodation). There is relaxation of the cilliary body and the suspensary ligament of the lens becomes tense. The lens becomes more concave and eye is fixed for far vision (Figure 2.3.2). Eye is unable to accommodate for the near vision and the near vision becomes blurred.
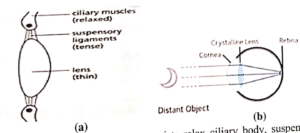
Figure 2.3.2. (a) Muscarinic M3 receptor antagonists relax ciliary body, suspensory ligaments become tense, and make lens more concave. (b) Eye is fixed for far vision.
c. Increase in intra-ocular pressure (IOP). Mydriasis and the relaxation of the cilliary body reduce the angle of anterior chamber of the eye and compress the Schlem’s canal. Thus reduce the drainage of the aqueous humor and increase IOP, which can precipitate glaucoma (Figure 2.3.3).
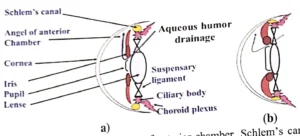
Figure 2.3.3. (a) Normal iris, pupil, angle of anterior chamber, Schlem’s canal and drainage of aqueous humor. (b) Pupil dilators (Muscarinic antagonists, e.g. Tropicamide) pull iris outwards, angle of anterior chamber is narrowed, Schlem’s canal (yellow) is pressed, drainage of aqueous humor is reduced and intraocular pressure is raised.
d. Xerophthalmia (dry eye), due to decrease in the secretions of the lacrimal glands.
Respiratory tract:
Block muscarinic M3 receptors on the bronchial tree and produce bronchodilatation. Due to the blockade of the parasympathetic effect, there is un-opposed sympathetic effect on the bronchi, leading to bronchodilatation.
Uro-genital tract:
Block muscarinic M3 receptors on the smooth muscle of bladder wall and trigone. Relax bladder and constrict trigone.
CVS:
Block muscarinic M2 receptors on the SA-node and produce tachycardia. When the parasympathetic action on SA-node is blocked, there is unopposed sympathetic action, leading to tachycardia.
Sweat glands:
Block muscarinic M3 receptors on the sweat glands cause decrease of sweating and increase in body temperature.
CNS:
a. Anti-Parkinsonism: Tertiary amine antimuscarinic drugs (e.g Benztropine and Procyclidine) can cross BBB, block excessive cholinergic activity in the basal ganglia, which occurs in the Parkinsonism due to damage to the inhibitory dopaminergic neurons in the substantia nigra of the basal ganglia in old age. Thus control the symptoms of Parkinsonism (Figure 2.3.4a).
[Note: The excess cholinergic activity in turn increases GABA-ergic inhibitory inputs to globus pellidus, thalamus, motor cortex and spinal cord. Besides there is also down regulation of Glutametergic excitatory inputs and abnormal oscillatory activity in the basal ganglia, leading to typical symptoms of Parkinsonism, i.e. bradykinesia, resting tremor and rigidity, with gradually worsening postural instability. The treatment includes antimuscarinic and dopaminergic drugs (Chapter 6.4)].
b. Anti-motion sickness: In motion sickness, excessive neuronal inputs from the labyrinth stimulate vomiting center and cerebellum. Thus produce nausea, vomiting and vertigo. Neuronal inputs from labyrinth to vomiting center and cerebellum are cholinergic, Antimuscarinic drugs (e.g. Hyoscine) counter these neuronal inputs and control symptoms of motion sickness (Figure 2.3.4b).
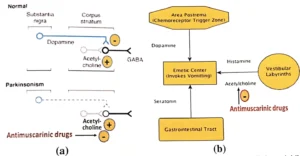
Figure 2.3.4. (a) Normal. Dopaminergic neurons from substantia niga (SN) have inhibitory control on neurons of corpus striatum. In Parkinsonism, this inhibitory control becomes weaker (Dashed line), due to age related deficiency of dopaminergic neurons in SN, causing uncontrolled excessive cholinergic activity. Antimuscarinic drugs (e.g. Procyclidine) control cholinergic activity. (b) In motion sickness, vestibular inputs from labyrinth to vomiting center are cholinergic, Antimuscarinic drugs (e.g. Hyoscine) control these neuronal inputs.
c. Other CNS effects: In usual doses Atropine causes stimulation and Hyoscine sedation. Over dosage of both causes delerium, convulsions and coma.
Uses:
GI:
a) Peptic ulcer: Pirenzepine is used which is more selective for decreasing HCl secretion.
b) Intestinal colic: Commonly used Antimuscarinic drugs are: i) Tertiary amines: Dicyclomine, Difemirine. ii) Quaternary amines: Hyoscine-butyl bromide, Propantheline & Glycopyrrolate.
Eye:
a) Endoscopic examination of the eye. Short acting antimuscarinic drugs (e.g. Tropicamide) are used topicaaly to dilate the pupil.
b) Rest to eye after injury or surgery. Longer acting antimuscarinic drugs (e.g. Atropine) are used to dilate the pupil. Because eye remains at rest when pupil is dilated. c) To prevent or break adhesions between iris and lense. In infection or injury to eye, thick secretions around the iris and lense tend to make adhesions on healing (due to fibrosis). To prevent these adhesions short acting mydriatic (e.g. Tropicamide) is used topically alternately with short acting miotic (e.g. Pilocarpine).
Respiratory tract: a) Asthma and chronic obstructive pulmonary disease (COPD). Ipratropium is used, which has more selective action on the bronchi. b) Pre-anesthetic medication. Atropine is used, which decreases secretions and prevents bronchoconstriction due to irritant effect of inhaled anesthetic agents.
Urogenital tract: Urinary urgency or incontinence. Oxybutinin is used, which has more selective action on bladder.
CVS: Sinus bradycardia and hypotension. Atropine is used to treat the sick-sinus syndrome.
Adverse effects: Overdose of anti-muscarinic drugs (Like Atropine) and poisoning due to Atropa belladonna and Dhatura stramonium (Figure 2.3.5). The signs and symptoms of poisoning include: Dry mouth, constipation, urine retention, tachycardia, blurring of vision, dryness of eyes and precipitation of glaucoma. Skin becomes hot and flushed and the body temperature increases. There is also sedation, confusion, loss of memory and delerium (Symptoms are more marked in the elderly).
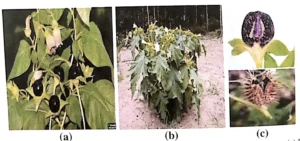
Figure 2.3.5. Plants containing Atropine; (a) Atropa belladona, (b) Dhatura stramonium, (c) Ripe fruits with seeds, Atropa belladonna (Top), Dhatura stramonium (Bottom).
Treatment: Symptomatic: Propranolol or another suitable beta-blocker (e.g. Atenolol, a cardioselective beta-blocker, in patients with asthma because propranolol, a cardionon-selective beta-blockers can cause bronchoconstriction) is given to control blood pressure and heart rate. Paracetamol is used to lower the body temperature and Diazepam for the convulsions. Specific: Physostigmine, a tertiary amine cholinomimetic drug, is given by slow IV injection, which reverses the peripheral and central nervous effects of atropine like drugs.
Contraindications: Glaucoma and enlarged prostate.
Oral & Dental Implications of Anticholinergic Drugs: a. Oral mucosal infiltrations of local anesthetic have the potential to induced vasovagal reflex. Which may be triggered by anxiety secondary to injection pain and fear. Vasovagal reflex can cause severe bradycardia and hypotension. Atropine is used to reverse the effects of vasovagal phenomenon. b. Long term use of anticholinergic drugs can cause persistent dry mouth, which may lead to dental-plaque, caries, and gingivitis. Particularly, when accompanied by poor oral hygiene. c. Anticholinergic drugs as such are not prescribed these days for long term use as they used to be in the past. However, some of the anti-psychotics (e.g. Chlorpromazine, Chlorprothixine and Thiothixine, etc.), anti-depressants (e.g. Tri-cyclic antidepressants, like Amitriptyline and Imipramine, etc.), anti-Parkinsonian drugs (e.g. Benztropine, Benzhexal and Procyclidine, etc.), and antihistamines (e.g. Diphenhydramine, Promethazine, etc.), which possess significant anti-muscarinic activity, are sometimes used for longer time and are likely to cause dry mouth and dental caries.